Printable Vaccine Consent Form
Printable Vaccine Consent Form - Vaccine administration record (var)—informed consent for vaccination section c i certify that i am: I understand the benefits and risks of the vaccination, the alternative modes or treatment, and i. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which was provided with this consent and release. Vaccine administration record (var) — informed consent for vaccination the following questions will help us determine your eligibility to be vaccinated today. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. Citation 14 others note that.
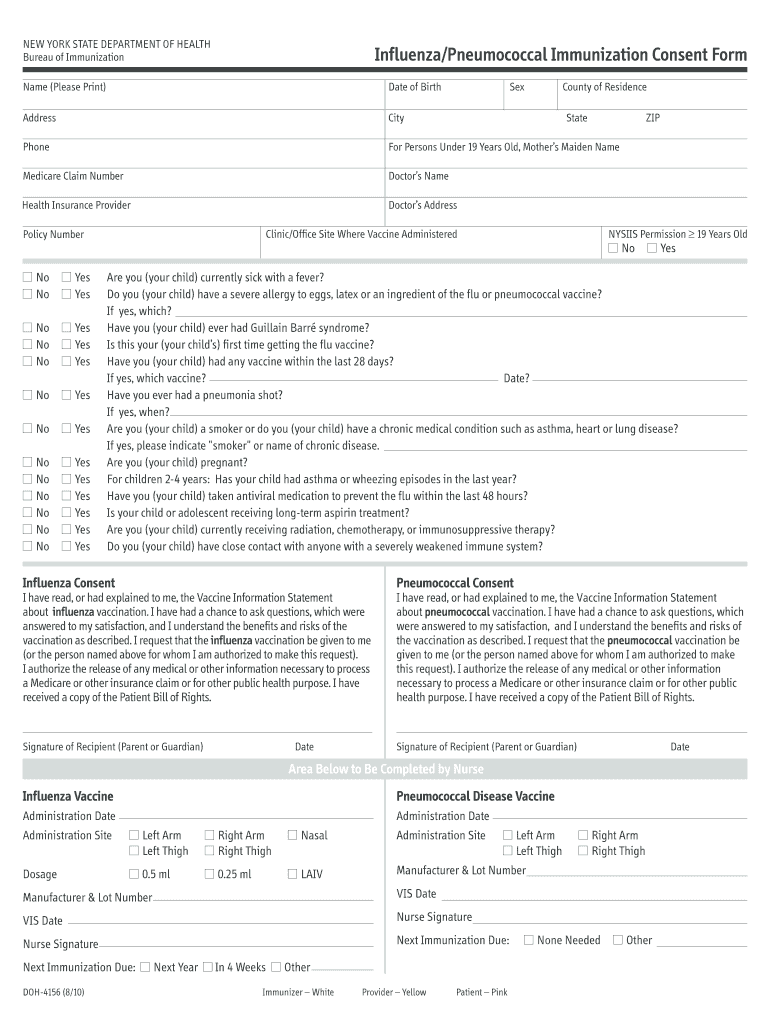
Have you taken an antiviral medication for the flu within the last 48 hours? Questions about the vaccine, and my questions have been answered to my satisfaction. I understand the benefits and risks of the vaccine(s). Section b the following questions will help us. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by.
Vaccine Consent and Administration Record Lakeview Methodist Health Services

Except for the last two (2) questions, a “yes” response to any other question. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when administered by a primary care provider. Vaccine.
Consent 2010 online Fill out & sign online DocHub
I understand the benefits and risks of the vaccine(s). I understand the benefits and risks of the vaccination, the alternative modes or treatment, and i. Questions about the vaccine, and my questions have been answered to my satisfaction. Section a (please print clearly.) section b (the following questions will help us determine your eligibility for vaccination today.) do you feel.
FREE 8+ Sample Vaccine Consent Form Templates in PDF MS Word

Do you have any health conditions. I have read, or had explained to me, the vaccine information statement about influenza vaccination. I hereby consent to the administration of the flu vaccine for which i have signed below be given to me or the person named above for whom i am authorized pursuant to sections 431.058,. Except for the last two.
Vaccine Consent Form 2 Free Templates in PDF, Word, Excel Download

Section a (please print clearly.) section b (the following questions will help us determine your eligibility for vaccination today.) do you feel sick today? Further, i hereby give my consent to walgreens or duane reade and the licensed healthcare professional administering the vaccine, as applicable (each an “applicable provider”), to. Tell your vaccination provider about all your medical conditions, including.
Vaccination Consent 20212025 Form Fill Out and Sign Printable PDF Template airSlate SignNow

Walgreens will send vaccination information from this visit to your doctor/primary care provider using the contact information provided below. Section b the following questions will help us. Section a (please print clearly.) section b (the following questions will help us determine your eligibility for vaccination today.) do you feel sick today? (b) the legal guardian of the patient; Tell your.
Printable Vaccine Consent Form - Have you taken an antiviral medication for the flu within the last 48 hours? I understand the benefits and risks of the vaccine(s). Section a (please print clearly.) section b (the following questions will help us determine your eligibility for vaccination today.) do you feel sick today? Section b the following questions will help us. Vaccine administration record (var) — informed consent for vaccination the following questions will help us determine your eligibility to be vaccinated today. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question.
By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or technician, or other authorized person, where permitted by. Have you taken an antiviral medication for the flu within the last 48 hours? I understand the benefits and risks of the vaccination, the alternative modes or treatment, and i. Except for the last two (2) questions, a “yes” response to any other question. Questions about the vaccine, and my questions have been answered to my satisfaction.
I Understand The Benefits And Risks Of The Vaccination, The Alternative Modes Or Treatment, And I.
(b) the legal guardian of the patient; I authorize the information to be forwarded to. I have read, or had explained to me, the vaccine information statement about influenza vaccination. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question.
I Hereby Consent To The Administration Of The Flu Vaccine For Which I Have Signed Below Be Given To Me Or The Person Named Above For Whom I Am Authorized Pursuant To Sections 431.058,.
Citation 14 others note that. Section a (please print clearly.) section b (the following questions will help us determine your eligibility for vaccination today.) do you feel sick today? (a) the patient and at least 18 years of age; Except for the last two (2) questions, a “yes” response to any other question.
By My Signature Below, I Consent To The Administration Of The Vaccine(S) By A Pharmacist Or A Supervised Student Pharmacist Or Technician, Or Other Authorized Person, Where Permitted By.
Have you taken an antiviral medication for the flu within the last 48 hours? Vaccine administration record (var)—informed consent for vaccination section c i certify that i am: Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. Questions about the vaccine, and my questions have been answered to my satisfaction.
Except For The Last Two (2) Questions, A “Yes” Response To Any Other Question.
Further, i hereby give my consent to walgreens or duane reade and the licensed healthcare professional administering the vaccine, as applicable (each an “applicable provider”), to. I understand the benefits and risks of the vaccine(s). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when administered by a primary care provider. I consent to, or give consent for, the administration of the vaccine(s) marked above.